

So you have initiated myopia treatment and had a successful control of a rapid progressor’s myopia. When should you stop myopia control treatment? Do you need to stop? What are the clinical considerations?
When does myopia stop progressing?
There is no firm consensus on when myopia stops progressing. The COMET study, Myopia stabilisation and associated factors among participants in the Correction of Myopia Evaluation Trial, suggested that the peak myopia deceleration of progression occured at around 12, and the mean age of myopia stabilisation was 15.5 years, with 48% of the cohort having stable myopia by 15. However the more myopic, and the younger the initiation of the myopia, the more rapidly and the longer the myopia progresses for with large variances based on ethnicity. COMET found that:
- 48% had stable myopia by age 15 years;
- 77% by age 18 years;
- 90% by age 21 years;
- By age 24 years, the curves of almost all of the participants, 96% had achieved the curve-based definition of myopia stabilization
Think of this in reverse – at age 15, half of myopes are still progressing, and it’s only at age 24 where almost all had stabilized.
Cho and Cheung conducted a study on when orthokeratology could be discontinued, for best myopia control results, as part of the Discontinuation of Orthokeratology on Eyeball Elongation (DOEE) study. They found that if OrthoK is ceased before 14 years of age, rapid progression similar to pre-OrthoK treatment can occur. As part of the study design participants wore OrthoK, stopped for two years, and then resumed. Results showed that whilst axial length elongation resumes once the treatment is stopped, stopping itself doesn’t cause a “rebound” or increased speed of growth. They have concluded that stopping lens wear for short periods of time like illness, or holidays, can be done safely. The authors concluded that orthokeratology lens wear should continue well beyond age 14, provided no adverse outcomes are occurring, and if treatment is stopped axial length should be closely monitored for at least six months after cessation.
In a study titled “Visual activity and its association with myopia stabilisation” Mitchell Scheiman and others found that 40% of fifteen year olds did not have myopia stabilisation. Spoiler alert: near work was found to potentially relate to how stable they were, however outdoor exposure was found to have no effects on stabilisation.

Axial Elongation in Myopic Children and its Association With Myopia Progression in the Correction of Myopia Evaluation Trial (COMET): Axial elongation and myopia progression by analysis cohort. Children who became myopic between 7-8 (younger cohort) had faster progression and a higher end result than children whose myopia initiated later (9-14). Both groups however had a similar myopic course, suggesting that myopia stabilisation may follow a pattern. The blue solid lines indicate axial length and the red dotted lines refraction outcomes.
Myopia progression beyond the teens
We have some data on late teen and young adult myopia progression. A retrospective study of myopia progression in adult single vision contact lens wearers aged 20-40 years by Bullimore et al found that 21% progressed by at least 1D over the 5 year study period.2
The longest follow up on this is a series of studies from Finland by Parssinen et al, who showed that mean myopia progression in the 20’s decade was -0.45 ± 0.71D. In almost half of cases, progression was ≥0.5D, and confirming the results of Bullimore et al a dozen years later, in 18% of cases myopia increased by ≥1.00 D.3
While most myopia stabilizes by the early-to-mid 20s, around 20% of young myopes in their 20s will still progress by at least 1D in that decade.
Why do you need to stop?
Perhaps you need to stop for cost reasons, eye health reasons, or patient compliance reasons. Common reasons we’ve encountered in clinical practice include:
- “She’s a teenager now and has gotten lazy with wearing her OrthoK lenses”
- “Can he stop wearing his soft contact lenses over school holidays?”
- “I have more than one child needing myopia management and need to work out where best to spend the time, effort and money”
- “These contact lenses are a bother to put on and take off each day; can he just wear glasses now?”
- “These eye drops are expensive and he says they sting – how much longer will we need to do this?”
Obviously, if there are genuine eye health concerns with a treatment – contact lens complications, solution or preservative allergies – these need to take priority. As for treatment ‘pauses’ due to laziness or school holidays, better compliance is generally linked to better myopia control results so treatment should ideally continue. If a treatment no longer suits the individual – for example a teen getting less sleep so inadequate treatment from OrthoK – think about switching treatments, in this case to multifocal soft contact lenses.
Family situations such as cost, which child ‘needs it most’ and even living situations between separated parents can all factor into selecting and continuing the best treatment – these will need individual consideration and sensitive clinical communication. Sometimes you may need to make the difficult choices between children in one family for cost of commitment reasons – younger children likely being the faster progressors – or to switch or stop plans where compliance or other factors simply make a treatment impossible. However, where possible:
The simplest clinical message is that myopia control treatments should ideally continue until the end of high school, and it would probably be best to see the child through further tertiary study before discontinuation too.
The second important clinical message is that myopia has to be corrected regardless, so if you’re using an optical treatment which both corrects and controls myopia, why stop?
Clinical considerations for cessation
We’ve established that half of young myopes will stabilize by age 15, meaning that the other half don’t. Ideally we want to continue treatment throughout childhood and even into the early 20s, and with optical treatments this is typically feasible. However if you need to discontinue treatment:
- Atropine cessation should be tapered.4 An example of a tapering schedule might be:
- Every other day for 2-3 months, then
- Once a week for 2-3 months.
- You may even consider additionally reducing concentration (eg. from 0.025% to 0.01%) for 2-3 months, maintaining the same dosage frequency and then reducing, if you feel a longer taper may be required.
If a child is old enough to discontinue atropine, are they old enough to consider switching to a contact lens treatment monotherapy instead?
- Switching from multifocal to single vision soft contact lenses could influence accommodation and binocular vision.5,6 Make sure to monitor for any near point symptoms which could affect comfort in young contact lens wearers with high visual demands, as is common in the late teens and early 20s with study
- Switching from OrthoK to daily soft contact lens wear could increase comfort issues. An OrthoK wearer who isn’t used to open-eye, all-day-long contact lens wear should be prepared for an adaptation phase.
- Teens and young adults7 can be visually symptomatic of changing from single vision contact lenses to multifocal contact lenses, suffering haloes and ghosting. This could be a consideration if you’ve discontinued OrthoK or multifocal CLs for single vision, noted myopia progression and encouraged return to multifocal CL wear.
The take home message
Each of your myopia control patients, and their families, can have individualized factors influencing their ability to start and continue with treatments. This involves clear communication at the outset that ideally myopia control treatments should continue throughout childhood and sensitive clinical communication to understand individual and family capacity.
If myopia control treatment is ceased before the end of childhood (age 18), it is important to monitor closely for any progression, and recommence some form of treatment if the myopia continues to progress. This might be every 3-6 months depending on the age of the child, their situation and your level of concern.
Young adult myopes wearing contact lens treatments may be happy enough to continue them even once myopia is stable.
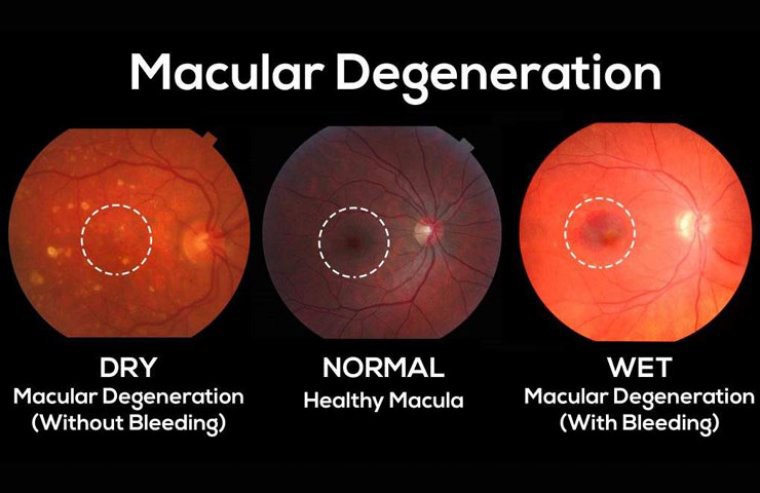
Finally, remember that myopia management doesn’t stop just because your patient has ceased myopia progression. Our adult myopes, especially those over 5-6D or with axial lengths longer than 26mm, will require close eye health monitoring throughout their lifetime due to their increased risk of macular and retinal disease.

Recent Comments